Irishcobs
Well-Known Member
I have had a few people ask about Inka's hock op so I thought I'd post a copy of her vet notes and pictures.
Inka was admitted to Donnington Grove Veterinary Surgery on 20th July 2011 for examination and treatment of a wound to the point of the right hind hock. Examination revealed that the calcaneal bursa (a synovial pouch at the back of the hock) was communicating with the wound. The degree of contamination of the calcaneal bursa meant that general anaesthesia, keyhole surgery and lavage was necessary.
The horse underwent a general anaesthetic and arthroscopic surgery with extensive lavage of the calcaneal bursa on the 21st July 2011. This revealed a laceration through approximately one third of the width of the superficial digital flexor tendon, establishing communication into the intertendinous calcanceal bursa. The bone at the point of the hock was exposed and curretage was carried out with the aid of an arthroscopic currette. The wound was cleaned and sutured with simple interrupted and tension relieving sutures. The horse recovered well from anaesthesia with the aid of a rope-assisted system. Post operatively Inka remained comfortable and the
wound sealed over adequately. A sample from the bursa revealed a white blood cell count not indicative of infection. Inka was treated with a combination of systemic and locally administered
antibiotics over the following days post surgery.
The sterile bandages should be maintained for two weeks post discharge. The wound should not discharge please consult with your veterinarian if concerned. The sutures should be removed in
two weeks from surgery. I have advised that Inka should have box rest for 6 weeks. A re-examination should be carried out before turnout into a very small paddock for 6 weeks, approximately half tennis court sized. During this time some walking exercise may also be commenced approx. 10 minutes twice daily. After this Inka may start a graduated return to full exercise over the following 3 months. The prognosis for Inka for a return to exercise is good. The details of the surgery are as follows:
On admission the pony was moderately lame with a laceration over the point of the right hock. A meaningful synovial fluid sample could not be obtained however a sample retrieved at the beginning of surgery revealed a high WBC on film with 74% Neutrophils and 26% Monocytes. The calcaneal bursa was pressure tested with saline and fluid freely exited from the wound. A bacterial culture and sensitivity revealed a scanty growth (Gram neg cocci - bacilli) on direct culture and a heavy growth Enterococcus faecalis which were both sensitive to trimethoprim sulfonamides. Radiographs did not reveal any significant bone abnormality.
Inka was given a general anaesthetic and positioned in dorsal recumbency. The limb was almost fully extended and supported by a custom rig. The right calcaneal bursa was examined tenoscopically. Portals were created both proximally and distally firstly on the medial aspect of the bursa. The portals on the lateral aspect of the limb were created morecentrally to allow
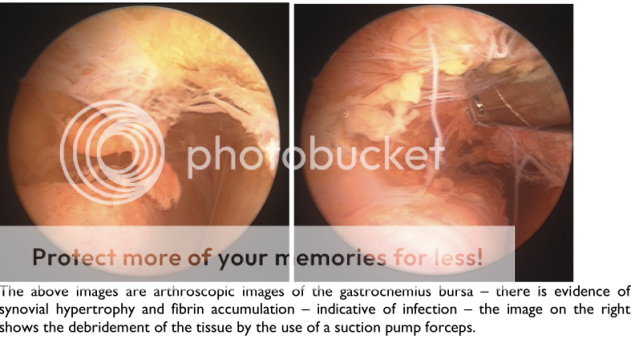
easier access to the wound so as to inspect and debride the tendon affected tendon, bone and wound. A 3cm transverse wound on the plantar aspect of the tuber calcis was freely communicating with the bursa. The intertendinous and gastrocnemius portions of the calcaneal
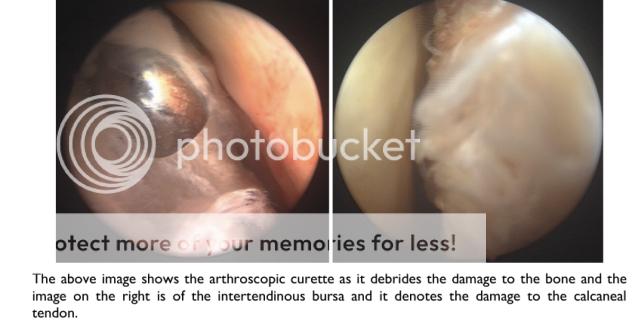
bursa demonstrated synovial hypertrophy and fibrin pannus accumulation. There was a small bone defect associated with the tuber calcis and curretage was carried out by the use of an arthroscopic currette. There was a laceration through the superficial digital flexor tendon on its
lateral aspect. The edges of the tendon were debrided using a suction punch forceps and motorized arthroscopic burr. The edges of the wound were sharply debrided and the wound was sutured using simple interrupted and vertical mattress sutures of 3.5 metric monofialment nylon. The bursa was lavaged extensively, medicated with 300mg amikacin and the tenoscopic
portals were closed routinely. The horse was recovered in a one layer Robert Jones bandage.
The following day the horse was walking quite comfortably. The limb was treated with 500mg amikacin by intravenous regional perfusion, and was then redressed using a presage bandage. A sample obtained before discharge under ultrasonographic guidance from the medial aspect of the calcaneal bursa whilst the limb was in passive flexion revealed a white blood cell count of WBC 9.2 x 109/l and a total protein of 62g/l.
Inka was admitted to Donnington Grove Veterinary Surgery on 20th July 2011 for examination and treatment of a wound to the point of the right hind hock. Examination revealed that the calcaneal bursa (a synovial pouch at the back of the hock) was communicating with the wound. The degree of contamination of the calcaneal bursa meant that general anaesthesia, keyhole surgery and lavage was necessary.
The horse underwent a general anaesthetic and arthroscopic surgery with extensive lavage of the calcaneal bursa on the 21st July 2011. This revealed a laceration through approximately one third of the width of the superficial digital flexor tendon, establishing communication into the intertendinous calcanceal bursa. The bone at the point of the hock was exposed and curretage was carried out with the aid of an arthroscopic currette. The wound was cleaned and sutured with simple interrupted and tension relieving sutures. The horse recovered well from anaesthesia with the aid of a rope-assisted system. Post operatively Inka remained comfortable and the
wound sealed over adequately. A sample from the bursa revealed a white blood cell count not indicative of infection. Inka was treated with a combination of systemic and locally administered
antibiotics over the following days post surgery.
The sterile bandages should be maintained for two weeks post discharge. The wound should not discharge please consult with your veterinarian if concerned. The sutures should be removed in
two weeks from surgery. I have advised that Inka should have box rest for 6 weeks. A re-examination should be carried out before turnout into a very small paddock for 6 weeks, approximately half tennis court sized. During this time some walking exercise may also be commenced approx. 10 minutes twice daily. After this Inka may start a graduated return to full exercise over the following 3 months. The prognosis for Inka for a return to exercise is good. The details of the surgery are as follows:
On admission the pony was moderately lame with a laceration over the point of the right hock. A meaningful synovial fluid sample could not be obtained however a sample retrieved at the beginning of surgery revealed a high WBC on film with 74% Neutrophils and 26% Monocytes. The calcaneal bursa was pressure tested with saline and fluid freely exited from the wound. A bacterial culture and sensitivity revealed a scanty growth (Gram neg cocci - bacilli) on direct culture and a heavy growth Enterococcus faecalis which were both sensitive to trimethoprim sulfonamides. Radiographs did not reveal any significant bone abnormality.
Inka was given a general anaesthetic and positioned in dorsal recumbency. The limb was almost fully extended and supported by a custom rig. The right calcaneal bursa was examined tenoscopically. Portals were created both proximally and distally firstly on the medial aspect of the bursa. The portals on the lateral aspect of the limb were created morecentrally to allow
easier access to the wound so as to inspect and debride the tendon affected tendon, bone and wound. A 3cm transverse wound on the plantar aspect of the tuber calcis was freely communicating with the bursa. The intertendinous and gastrocnemius portions of the calcaneal
bursa demonstrated synovial hypertrophy and fibrin pannus accumulation. There was a small bone defect associated with the tuber calcis and curretage was carried out by the use of an arthroscopic currette. There was a laceration through the superficial digital flexor tendon on its
lateral aspect. The edges of the tendon were debrided using a suction punch forceps and motorized arthroscopic burr. The edges of the wound were sharply debrided and the wound was sutured using simple interrupted and vertical mattress sutures of 3.5 metric monofialment nylon. The bursa was lavaged extensively, medicated with 300mg amikacin and the tenoscopic
portals were closed routinely. The horse was recovered in a one layer Robert Jones bandage.
The following day the horse was walking quite comfortably. The limb was treated with 500mg amikacin by intravenous regional perfusion, and was then redressed using a presage bandage. A sample obtained before discharge under ultrasonographic guidance from the medial aspect of the calcaneal bursa whilst the limb was in passive flexion revealed a white blood cell count of WBC 9.2 x 109/l and a total protein of 62g/l.